internship assesment-online blended assesment
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
Hii,
I am S.ShivaniReddy posted in general medicine under unit 3 .In these blog am sharing my research based learning and my experiences in internship

Unit duty:(13/7/23 to 11/8/23)
The following 4 weeks I was posted in the general medicine unit 3. Here we would have OP days and casualty duties with an occasional Sunday duty which made me realise that a good clinician has no days off.
AUDIT DUTY:
The best part of unitduty is audit.I found it very exciting.The main aim of this audit duty is PATIENT INTERACTION.The crux of this audit is extracting as much patient data as possible by asking there daily routine/change in the daily routine due to disease and adding those inputs to diagnose their condition.I did 4 audit duties ,interacted with 50 patients ,asked their daily routine and extracted very crucial data and it helped in diagnosing the patients condition.Typing whole data of the patient in audit gave me a basic idea of the patient ,his vitals.I did systemic examination on every audit patient in OP.It helped me improve my clinical knowledge.
PAJRs and blogs:
Importance of PAJR(Patient Journey Record System):
Machine learning. The PaJR system applied machine learning methods to predict patient status in the near future from data entered into the PaJR system. Given that points of contact with patients are frequent, individual points of contact with patients were used to model the flow of time: in predicting the status of a variable at some future point, an estimate was made of the value of that variable at the time of the next call. The predictions are based on information obtained at the current call, past calls to the patient and calls to all other participating patients. The predictive capacity is available to all of the monitored variables (e.g. whether, by the next point of contact, medication will have been taken as directed or an unplanned visit to an emergency room will have been made, and so on). The method generalized (with loss of certainty) to calls at points further into the future than the next call. In our study, values of three target variables statuses served as proxy measures of near-future patient status: next urgent unplanned events (NUUE), next unplanned events (NUE) and next self-rated health (next SRH). Patient baseline records and daily online interview logs (the PaJR system phone call summaries) deliver rich information about patients’ current status. Linguistic and meta-linguistic features are extracted together with current patient status, in order to train prediction models. The patient status prediction system is constructed in two phases, and it responds to requests in nearly real time. The two phases are offline training module and online prediction module. The offline training module utilizes the newest patient interviews and re-trains decision models within a few hours, while the online prediction module runs over the latest successful model, and it takes only moments to deliver prediction results https://www.researchgate.net/figure/Machine-learning-The-PaJR-system-applied-machine-learning-methods-to-predict-patient_fig1_229433689.
I created around 9 PAJR groups and updated critical data about the patient like his ECG ,Chestxray,2decho,feverchart and important points which could help us in diagnosis and treatment of patient.
PAJR mainly consists of blogs and soapnotes
SOAP NOTES:
Soap notes consist of complaints,vitals,diagnosis and treatment of patient which are upadated daily in PAJR group according to patients reports and condition.I updated 20 soap notes of my patients in PAJR groups
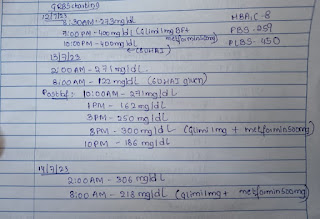
FEVER CHART:
In medicine department my pgs taught me how to plot fever chart,importance of fever chart .
BLOGS:
BELOW ARE THE LINKS OF MY BLOGS:
http://shivanireddymedicalcasediscussion.blogspot.com/2023/07/a-60-year-old-male-with-sob-since-6.html
http://shivanireddymedicalcasediscussion.blogspot.com/2023/08/a-19ym-with-pyrexia-under-evaluation.html
http://shivanireddymedicalcasediscussion.blogspot.com/2023/07/a-57ym-with-co-of-stiffness-of-bl-upper.html
http://shivanireddymedicalcasediscussion.blogspot.com/2023/08/a-60-yr-old-female-with-facial-puffiness.html
http://shivanireddymedicalcasediscussion.blogspot.com/2022/03/psoriasis.html
http://shivanireddymedicalcasediscussion.blogspot.com/2022/02/a-60-yearold-male-with-pain-abdomen.html
http://shivanireddymedicalcasediscussion.blogspot.com/2022/01/a-60-year-old-male-presented-to-opd.html
I had come across several patients during this period. Some critical coming from casualty and some not as much. We would take the critical ones to the ICU after stabilising them in the ICU we would shift them to ward.
Camp cases:
Daily we would admit 3 cases in our unit,get all the necessary investigations done and take proper history and treat them and discharge them .
PERIPHERALS:(13/6/23 to 27/6/23)
These days were particularly challenging as you are surrounded with critical patients and you never know when one may deteriorate.
It was an amazing experience spending time here. What I learned here includes:
NEPHROLOGY DUTY
Nephrology duties were slightly calmer than the ICU days but we did have a few emergencies coming in at odd hours.
A list of things which experienced and learned here include:
WARD DUTY
Ward days were relatively easy going days during the peripherals as we had all of the stable patients here.
What I learned here includes:
PSYCHIATRY (28/6/23 to 12/7/23):
During the initial 15 days, I was posted in the department of Psychiatry.
Here I learned about the importance of taking a detailed history of a patient from what they remember of their childhood to the current time to draw a definitive diagnosis.
A few cases that I’ve come across during this period include:
We learnt in detail about classifications of different psychiatric conditions, and the treatment of choice in each case.
We also got a chance to observe cases in the de-Addiction centre, and counsel the patients undergoing therapy.